博文
Fatal Household Transmission of Human Adenovirus Type 55
|||
Human Adenovirus Type 55 Causes Fatal Acute Respiratory Disease with Household Transmission. Emerg Infect Dis. 2019, 25(9): 1754-1756. 警惕人呼吸道腺病毒的近距离高传染性!

Human adenoviruses are associated with mild and acute respiratory infections, depending on the virus type and host immunity. Human adenovirus type 55 (HAdV-55) (1), formerly known as HAdV-11a (2), is a reemergent respiratory pathogen that has caused severe pneumonia outbreaks in military and civilian populations in Europe and Asia (2–7). However, household transmission of HAdV-55 is rarely reported. We report a case of household transmission of HAdV-55 involving 3 confirmed adult cases with 1 death. Epidemiologic, clinical, and laboratory investigations, along with whole genome sequencing, elucidate the disease progression and the pathogen origin.
During April 1–May 5, 2012, 7 household members (5 males and 2 females; 3 children and 4 adults) in Anhui Province, China sequentially experienced influenza-like symptoms, including fever, productive cough, fatigue, pharyngalgia, dyspnea, and other symptoms. The youngest patient was 4 months of age, the oldest, whom we refer to as AQ-1, was a 55-year-old man. The family lived together near a farm in a house with poor sanitary and ventilation conditions.
The first onset of acute respiratory disease (ARD) occurred on April 1, when the index case, a 4-year-old granddaughter of AQ-1, had a febrile respiratory infection with cough. Three days later, AQ-1’s grandson, 1 year of age, displayed similar symptoms. On April 9 and 11, AQ-1’s daughter, 28 years of age, and another grandson, 4 months of age, both had influenza-like symptoms. On April 14, AQ-1 had a fever, chills, and lumbago. He was admitted to the hospital on April 14 where clinicians diagnosed pneumonia. AQ-1 had close contact with his sick grandsons and granddaughter and had not been out of the house during the month he cared for them.
While hospitalized, AQ-1 had bilateral pneumonia seen on chest computed tomography (CT), temperature of 41.0°C, and low total leukocyte (3.63 × 109/L) and platelet (42 × 109/L) counts. AQ-1 sustained high fever and yellow phlegm despite anti-inflammatory and antiviral treatment, including levofloxacin, piperacillin sodium, tazobactam sodium, and ribavirin.
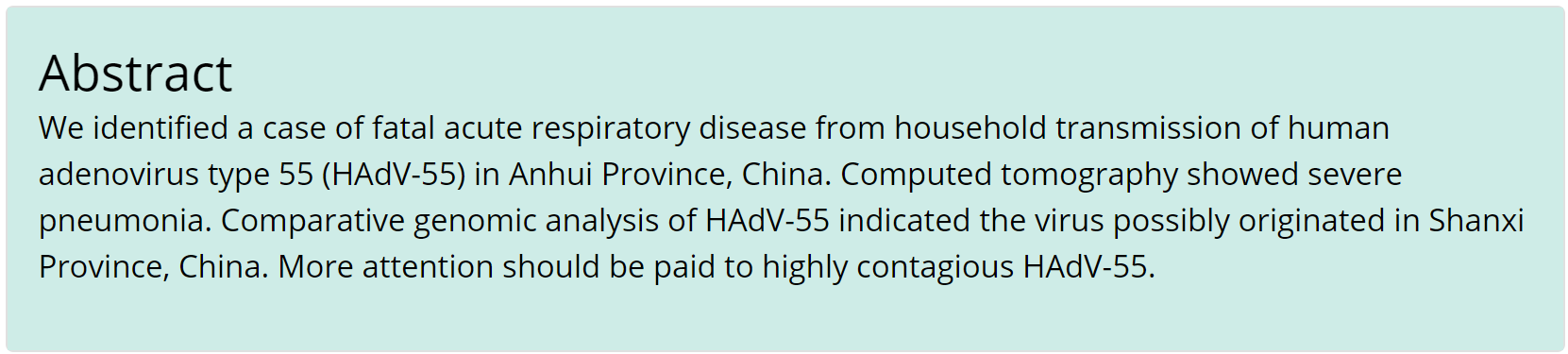
On April 24, AQ-1 had indications of severe pneumonia, including respiratory failure, hypoxemia, double lung rales, and a mass of shadows visible on chest CT. In addition, he had indications of liver damage and multi-organ failure. Transverse chest CT images demonstrated increased areas of patchy shadows and consolidation in both lungs compared to CT images from April 22, indicative of disease progression (Appendix Figure 1).
Appendix Figure 1. Chest computed tomography (CT) findings of case-patient AQ-1 who died from acute respiratory disease associated with human adenovirus 55 infection. A) and B) Upper and lower chest fields on April 22, day 8 after illness onset. Transverse CT images in the parenchymal window show ill-defined patchy and ground-glass opacities in all lobes of right lung and upper lobe of left lung and consolidation of lower lobe in left lung, suggestive of inflammatory exudation changes. Air-bronchogram can be found within the consolidation area. Note the slightly thickened right-sided pleura. C) and D) Upper and lower chest fields on the case-patient on April 24, day 10 after illness onset. The corresponding transverse CT images in the parenchymal window demonstrate increased areas of patchy opacities and consolidation in the bilateral lungs, as well as more obviously thickened right-sided pleura, indicative of the progression of disease.
AQ-1 died on April 27, 3 days after onset of respiratory failure, and 13 days after his illness began. On the same day, his 20-year-old son, AQ-2, and 31-year-old nephew, AQ-3, who had taken care of AQ-1 for 5 days, also exhibited symptoms of influenza-like illness. Both were hospitalized and had normal chest CT scans, but AQ-2’s leukocyte count was 5.4 × 109/L and AQ-3’s was 6.7 × 109/L. After antiinflammatory and antiviral treatment, including vitamin C, sulbactam, amoxicillin, amikacin, cefoperazone, ribavirin, and oseltamivir, they recovered and were discharged on May 5 (Figure).

We tested endotracheal aspirates from AQ-1 and throat swabs from AQ-2 and AQ-3 for influenza A and B viruses, severe acute respiratory syndrome coronavirus, human metapneumovirus, rhinoviruses, parainfluenza viruses 1–4, and HAdVs by real-time PCR. Only adenovirus was strongly positive for all the 3 patients. The antibodies against Mycoplasma pneumoniae, Mycobacterium tuberculosis Treponema pallidum, hepatitis B and C viruses, and HIV, all were negative. After treatment, samples from AQ-2 and AQ-3, were negative for adenovirus by PCR.
We isolated AQ-1’s adenovirus in culture and sequenced the genome (GenBank accession no. KP279748). Sequences for the hexon, penton base, and fiber genes were identical to those previously reported for HAdV-55. Phylogenetic analysis showed that the 3 isolates clustered closely with other strains from China (Appendix Figure 2). The genome of AQ-1’s strain had the highest nucleotide identity (99.951%) with QZ01_2011, an isolate from a military trainee in Shanxi Province, China. The second highest identity (99.948%) was with QS-DLL_2006, which caused a fatal ARD outbreak in a senior high school in Shaanxi Province, China (1, 8) (Appendix Table). We hypothesize the strain infecting AQ-1 and his family originated from Shanxi Province.


Appendix Figure 2. Phylogenetic analysis of human adenovirus 55 (HAdV-55) strain AQ-1_2012 from a fatal case of household transmission of HAdV-55, Anhui Province, China, 2012. Nucleotide sequences of archived HAdV-55 genomes retrieved from GenBank (https://www.ncbi.nlm.nih.gov/genbank) are used for comparison. Sequence names include GenBank accession number, isolation country, strain name, and year of isolation. Phylogenetic trees were constructed in MEGA7.1.0 (https://www.megasoftware.net) by using maximum-composite-likelihood method and applying default parameters with 1,000 bootstrap replications. Bootstrap proportions are shown as numbers on branches and at nodes. HAdV-C1 is included as an outgroup. Scale bar indicates number of nucleotide substitutions per site; ▲, indicates sequence from the case referenced.
In this household transmission of ARD, the index case was a probable case because no specimens were collected to confirm virologic identification. From the timeline of illness onset in this household cluster of ARD cases (Figure), we suspect that the pathogen spread rapidly among the children and further circulated in adults who had close contact with infected children and one another.
HAdV-55 contains a 97.4% genome of HAdV-14 and a hexon from HAdV-11 (1). Since 2006, HAdV-14 has caused severe ARD in America, Europe, and Asia (8,9), with high hospitalization (38%) and case-fatality (5%) rates (10). Because the risk for infection among the close contacts may rise, more attention should be paid to these highly contagious pathogens.
Ms. Jing was a graduate student at Southern Medical University and works at Zhuhai Center for Disease Control and Prevention, Guangdong Province, China. Her research interest is the epidemiology of human adenoviruses. Jing Zhang is a PhD candidate at Southern Medical University, Guangzhou, China, whose primary research interests are genomics and evolution of human adenoviruses.
Acknowledgment
This study was approved by the institutional review board of Anqing Center for Disease Control and Prevention and was supported by the National Natural Science Foundation of China (grant nos. 31570155, 31370199, 81730061, 81471942) and Guangzhou Healthcare Collaborative Innovation Major Project (grant nos. 201803040004, 201803040007).
References
1. Walsh MP, Seto J, Jones MS, Chodosh J, Xu W, Seto D. Computational analysis identifies human adenovirus type 55 as a re-emergent acute respiratory disease pathogen. J Clin Microbiol. 2010;48:991–3.
2. Kajon AE, Dickson LM, Metzgar D, Houng HS, Lee V, Tan BH. Outbreak of febrile respiratory illness associated with adenovirus 11a infection in a Singapore military training cAMP. J Clin Microbiol. 2010;48:1438–41.
3. Cao B, Huang GH, Pu ZH, Qu JX, Yu XM, Zhu Z, et al. Emergence of community-acquired adenovirus type 55 as a cause of community-onset pneumonia. Chest. 2014;145:79–86.
4. Salama M, Amitai Z, Amir N, Gottesman-Yekutieli T, Sherbany H, Drori Y, et al. Outbreak of adenovirus type 55 infection in Israel. J Clin Virol. 2016;78:31–5.
5. Lafolie J, Mirand A, Salmona M, Lautrette A, Archimbaud C, Brebion A, et al. Severe pneumonia associated with adenovirus type 55 infection, France, 2014. Emerg Infect Dis. 2016;22:2012–4.
6. Heo JY, Noh JY, Jeong HW, Choe KW, Song JY, Kim WJ, et al. Molecular epidemiology of human adenovirus-associated febrile respiratory illness in soldiers, South Korea. Emerg Infect Dis. 2018;24:1221–7.
7. Zhu Z, Zhang Y, Xu S, Yu P, Tian X, Wang L, et al. Outbreak of acute respiratory disease in China caused by B2 species of adenovirus type 11. J Clin Microbiol. 2009;47:697–703.
8. Carr MJ, Kajon AE, Lu X, Dunford L, O’Reilly P, Holder P, et al. Deaths associated with human adenovirus-14p1 infections, Europe, 2009-2010. Emerg Infect Dis. 2011;17:1402–8.
9. Huang G, Yu D, Zhu Z, Zhao H, Wang P, Gray GC, et al. Outbreak of febrile respiratory illness associated with human adenovirus type 14p1 in Gansu Province, China. Influenza Other Respir Viruses. 2013;7:1048–54.
10. Centers for Disease Control and Prevention (CDC). Acute respiratory disease associated with adenovirus serotype 14—four states, 2006-2007. MMWR Morb Mortal Wkly Rep. 2007;56:1181–4.
https://blog.sciencenet.cn/blog-51164-1194144.html
上一篇:2019年国自然基金委仅支持6项腺病毒相关研究项目?看着今年这么多重症腺病毒肺炎的患儿,感叹我们基础研究的薄弱
下一篇:美国科普作家Michael Coston Highlighted EID paper:人55型腺病毒引起致死性家庭传播